Anatomy Corner: Iliotibial Band
The iliotibial band is a band of fascia, made up of thick connective tissue containing collagen and a little bit of elastin. The collagen fibers are very strong, making the ITB a tough band of fascia, and the elastin provides some elasticity (hence the name, elastin).
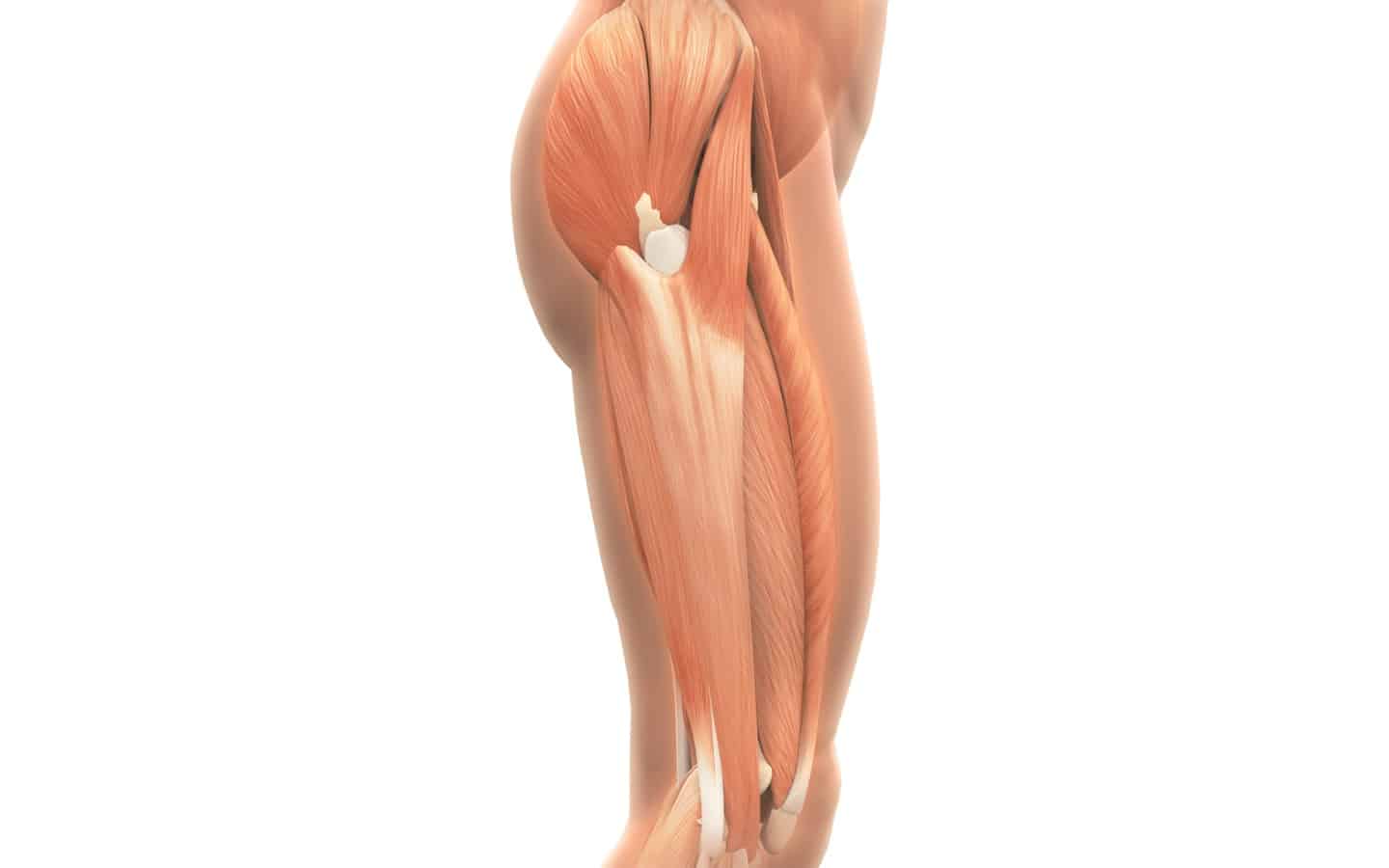
The ITB runs from the top of the pelvic bone, along the iliac crest, connecting with the superficial fascia of the gluteus medius, gluteus maximus, tensor fasciae latae, and the vastus lateralis. The ITB attaches to the lateral tibia, but there are also fibers from the ITB that run medially and along the anterior patella. This makes it difficult for the patella to glide medially.
One misconception about the ITB is that it works like a muscle, having the ability to contract and tighten. However, the ITB is a static hip and knee stabilizer, and does not have the ability to contract like a muscle, because it is made of connective tissue, a non-contractile tissue. However, the muscles that attach to the ITB can contract and tighten. The ITB can become adhered to the fascia, which attaches the muscle to the ITB.
Foam rolling the ITB has always been a first line of defense to treat ITBS. Foam rolling can be very effective for helping tight muscles by increasing circulation and loosening up tight tissue. In order to help relieve pain due to ITBS, or prevent ITBS, foam rolling the muscles that are connected to the ITB can help.
Foam rolling directly over the ITB will not help and may actually irritate the ITB more. Focus on foam rolling over the lateral quadriceps, the lateral hamstrings, and the glutes. (The tensor fasciae latae is a difficult muscle to roll over, due to its close proximity to the anterior pelvic bone.) Follow up with stretching the tight muscles that are connected to the ITB-the lateral quadriceps, lateral hamstrings, and the glutes.
Common injuries that involve the ITB are: ITBS, snapping hip, snapping knee, and trochanteric bursitis. All the diagnoses above have to do with the ITB pressing or rubbing on a bony prominence or on the bursal sac, causing inflammation and pain. However, the ITB can also pull the patella laterally, due to tightness in the lateral muscles, and/or a muscle strength imbalance between the medial and lateral muscles of the LE, which can cause pain in the knee.
ITB pain can present in the lateral hip, lateral knee, or anterior knee due to the iliotibial band. Always see a physical therapist to help diagnose the cause of pain, rule out other possible pathologies, and provide a treatment plan.
By Aubin Sullivan